

Introduction
Implant success is largely dependent on achieving high primary stability upon placement. However, this is made difficult in an atrophic jawbone. In particular, reduced vertical bone height in the maxilla makes implant placement challenging. The sinus lift procedure has been utilised for several decades as a way of creating more space and facilitating bone augmentation in order to allow primary stability of placed implants. Both one- and two-stage surgeries have been described in the literature. Success of these procedures, both in terms of graft and implant survival rates, is shown to be high. There is also evidence that a grafted sinus lift affords greater vertical bone height gain than non-grafted surgeries.
Though an autogenous bone graft material is viewed to be the gold standard and offers a potentially quicker healing time, the drawbacks of a second surgical site are less than ideal for many patients. Bone substitutes, therefore, offer an alternative that many patients and practitioners prefer, offering comparable clinical and radiological results. The following case demonstrates the successful implementation of using 100 per cent allograft during a bilateral sinus lift procedure, with delayed implant placement after a six-month healing period.
Case presentation
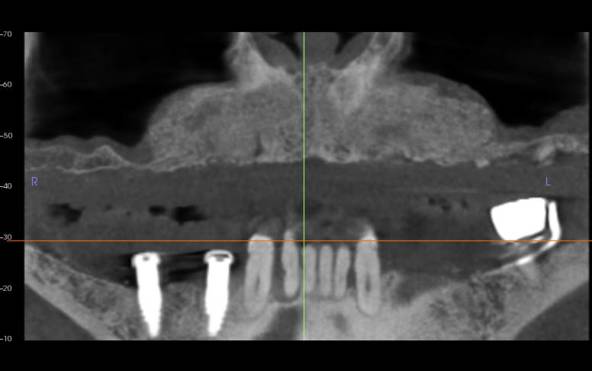
A male patient was referred by his routine clinician for implant treatment in the upper arch. He presented with a minimally retentive upper denture that was held in place by two grade III mobile canine teeth. The patient had already received two implants in the lower jaw that were retaining the lower denture with locators and, due to the success of this procedure, he was interested in something similar for the upper arch.
A comprehensive clinical assessment was conducted, including a full medical history and evaluation of the soft tissue, occlusal vertical dimension and freeway space. The denture was also assessed to determine whether it could be used to fabricate the new implant-retained prosthesis. A fractured incisor tooth had recently been extracted, leaving a relatively fresh extraction socket at the UR1 site. With regards to lifestyle factors, the patient was a regular smoker. However, he agreed to stop a month before surgery and remain smoke-free at least for the duration of the surgical phase of treatment but was made well aware of the increased failure rate with smokers.
Treatment planning
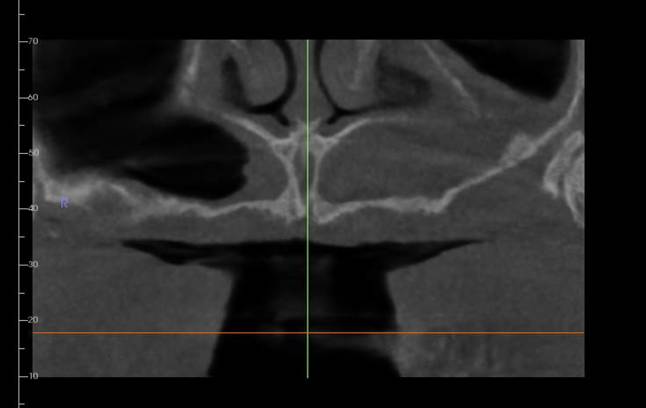
A full suite of diagnostic images was taken, including a CBCT to assess the underlying bony infrastructure. Bilateral sinus lifts were indicated in order to place implants for an implant-retained denture. Two infected canines would also require extraction.
The soft tissue was also assessed for mucosa health and volume, smile line, as well as the sulcus depth and keratinised mucosa, determining whether soft tissue grafting would be necessary and if any other challenges should be anticipated during treatment.
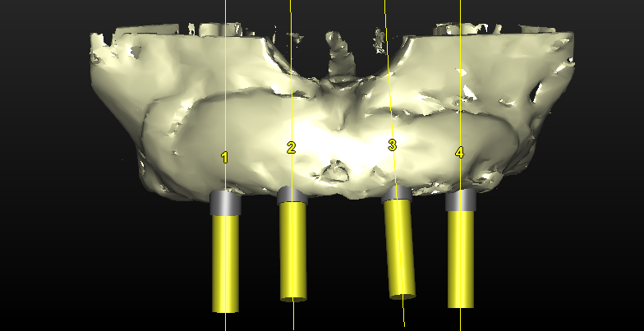
Surgical treatment was digitally planned using Simplant software and a bone supported placement guide was made based on what was established to be the ideal implant position. The patient was informed that during the healing time, he would not wear the denture for three months to prevent pressure on the grafted area. A new CBCT would be taken after four months of healing following the sinus lift procedure. The implants would be then placed and another four months allowed before the restoration phase began.

Surgical treatment
The bilateral sinus lifts were performed in two sessions, approximately two weeks apart. In each situation, the same procedure was followed. Local anaesthesia was administered and a flap raised. The sinus membrane was elevated and 3.5-5cc of MinerOss from BioHorizons Camlog was placed into the site with the intention of not only creating bone vertically, but also horizontally. An allograft material was ideal as there was minimal autogenous bone present in lower jaw, making harvesting adequate autogenous bone difficult – especially considering that the amount of graft material needed was more than what could be gathered from a single ramus or the chin. The patient also expressed a preference to avoid another surgical site. In addition, MinerOss provides rapid bone conversion to vascularised bone to allow for successful implant placement within the following months. This is preferable than when using xenograft or other synthetic grafting materials.
The soft tissue was closed over the surgical site and sutured without tension. Standard post-operative instructions were given to the patient to protect the site during initial healing and encourage excellent oral hygiene. This meant avoiding chewing in the area and regularly using an antimicrobial mouthwash. The patient was delighted with the initial outcome achieved and the importance of his smoking cessation was emphasised.
Review and reflection
Sinus lifts are advanced procedures that should be approached only when the clinician has sufficient training and experience. Adding to the complexity in this case was the extremely large size of the sinus lift, which extended from the molar sites to the incisive canal in the midline.
Another difficult aspect of this treatment was provisionalisation – the graft was extensive and could not come under any pressure while healing to avoid resorption. As well as this, it was important to place enough graft material to allow decent distribution of the implants placed while also maintaining height and width of bone around the implants. The sinus lifts were performed within two weeks of each other to allow the patient to chew on one side at a time. This was why it was important to avoid denture wear for at least three months during the healing process.
The case also reflects why graft material selection is crucial. I have been using MinerOss for four to five years because the cortical component in the granules leads to very little bone resorption, while the cancellous particles promote revascularisation. It gives a much better tissue response with healing compared to other solutions – it does not get incorporated into the surrounding soft tissue and periostem, making second stage surgery neater as the mucosa lifts from the bone easily for effective soft tissue manipulation. MinerOss also exhibits simple handling, especially when mixed with blood, and I use it confidently in any case that requires grafting.
References available on request.
For more information visit https://theimplanthub.com/